Program

CME Accreditation
12th International Winter Arrhythmia School was approved for the following credits by Continuing Professional Development, Faculty of Medicine, University of Toronto:
Royal College of Physicians and Surgeons of Canada – 17.5 Section 1 credits
The American Medical Association – 17.5 AMA PRA Category 1 credits
The College of Family Physicians of Canada – 4.0 Mainpro-M1 credits
Through an agreement between the Royal College of Physicians and Surgeons of Canada and the American Medical Association, physicians may convert Royal College MOC credits to AMA PRA Category 1 Credits™. Information on the process to convert Royal College MOC credit to AMA credit can be found at www.ama assn.org/go/internationalcme.
12th International Winter Arrhythmia School was endorsed by:
Workshops
Building on the success of previous conferences, our workshops offered specialized instruction for nurses, EP technicians, residents, fellows, and allied professionals.
We deployed world-class faculty to engage in discussions and expect, as always, fierce educational argument.
International Winter Arrhythmia School Founder and Chair: Dr. Eugene Crystal
12th Annual Hosting Faculty
12th Annual International Faculty
|
12th Annual National Faculty
|
Organizers Banafsheh Arouny & Seddigheh Baktash
Supporting Organizations
We are grateful to the following partners for their generous support of last year’s International Winter Arrhythmia School:
12th International Winter Arrhythmia School is endorsed by:
2015 Sponsors:
Location
The 12th International Arrhythmia School was hosted at the Westin Trillium House at Blue Mountain in Collingwood, Ontario. Blue Mountain is a ski resort located approximately 90 minutes by car outside of Toronto. 220 Gord Canning Drive (Formerly Mountain Drive), Blue Mountains Ontario, L9Y 0V9, Canada Phone: (705) 443-8080
Abstracts
Harrington Heart and Vascular Institute, University Hospitals Case Medical Center, Case Western Reserve University, School of Medicine, Cleveland, Ohio, USA
Abstract:
Purpose: This pilot study was designed to assess the feasibility and safety of using the Stereotaxis and the AmigoTM Remote Catheter System (RCS) as a non-fluoroscopic approach for EGM-guided atrial fibrillation (AF) ablation.
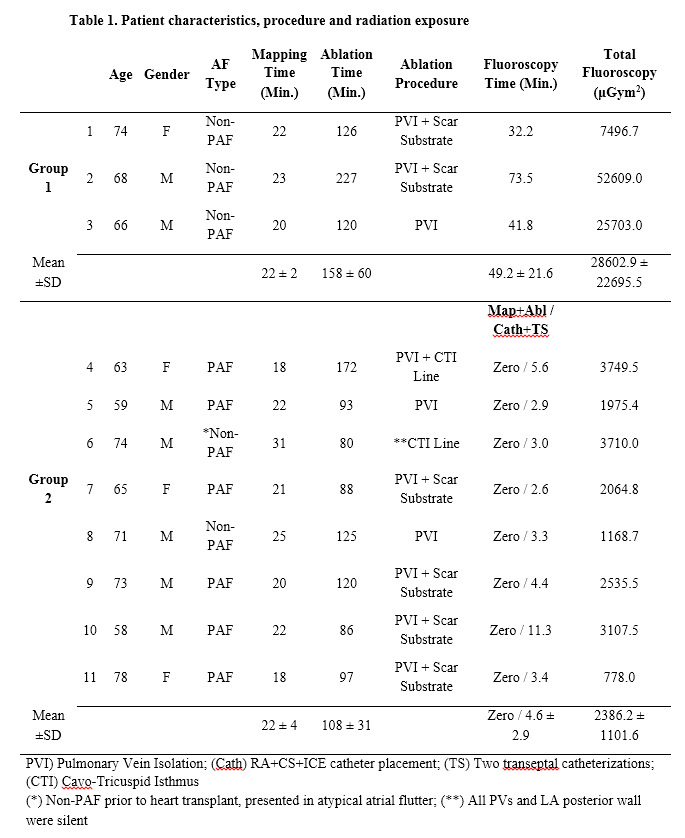
Methods: This prospective study enrolled 11 consecutive patients presenting for radiofrequency (RF) catheter ablation of AF. Group 1. The initial 3 patients underwent 3-D electroanatomic voltage mapping while creating LA and PV antra geometry. This was obtained by roving a custom, bidirectional multi-electrode circular catheter remotely via the Amigo RCS. Subsequently, PV electrical isolation (PVI) and adjunctive ablation was performed by remote RF delivery via the Stereotaxis magnetic system. This phase was designed to allow the operator to become familiar with the Amigo remote navigation and fluoroscopy was allowed as needed. Group 2. The subsequent 8 patients underwent the same procedure to test the following hypothesis: “A fully robotic EGM-guided AF ablation can be performed without or minimal radiation exposure”.
Results: All 11 patients underwent successful robotic EGM-guided PVI, scar substrate and CTI ablation, as needed using the Stereotaxis and the Amigo RCS systems. In all patients in Group 2, LA and RA mapping (22 ± 4 min.) and ablation (108 ± 31 min.) were performed without fluoroscopic. The mean fluoroscopic time and total radiation exposure (μGym2) was 49.2 ± 21.6 vs. 4.6 ± 2.9 min., and 28602.9 ± 22695.5 vs. 2386.2 ± 1101.6 μGym2 for Group 1 and Group 2, respectively (P < 0.001). There were no complications and AF recurred in 1 patient during short-term follow-up (99-126 days).
Conclusion: This pilot study suggests that a fully robotic EGM-guided AF ablation and adjunctive ablation can be performed safely and with minimal radiation exposure.
Table 1. Patient characteristics, procedure and radiation exposure
Presentation Downloads
ECG Workshop by Dr. A. Baranchuk & Dr. K. Quinn
ECG in Cardiac Devices by Dr. A. Pinter
ICD Troubleshooting (case-based) by Dr. A. Pinter
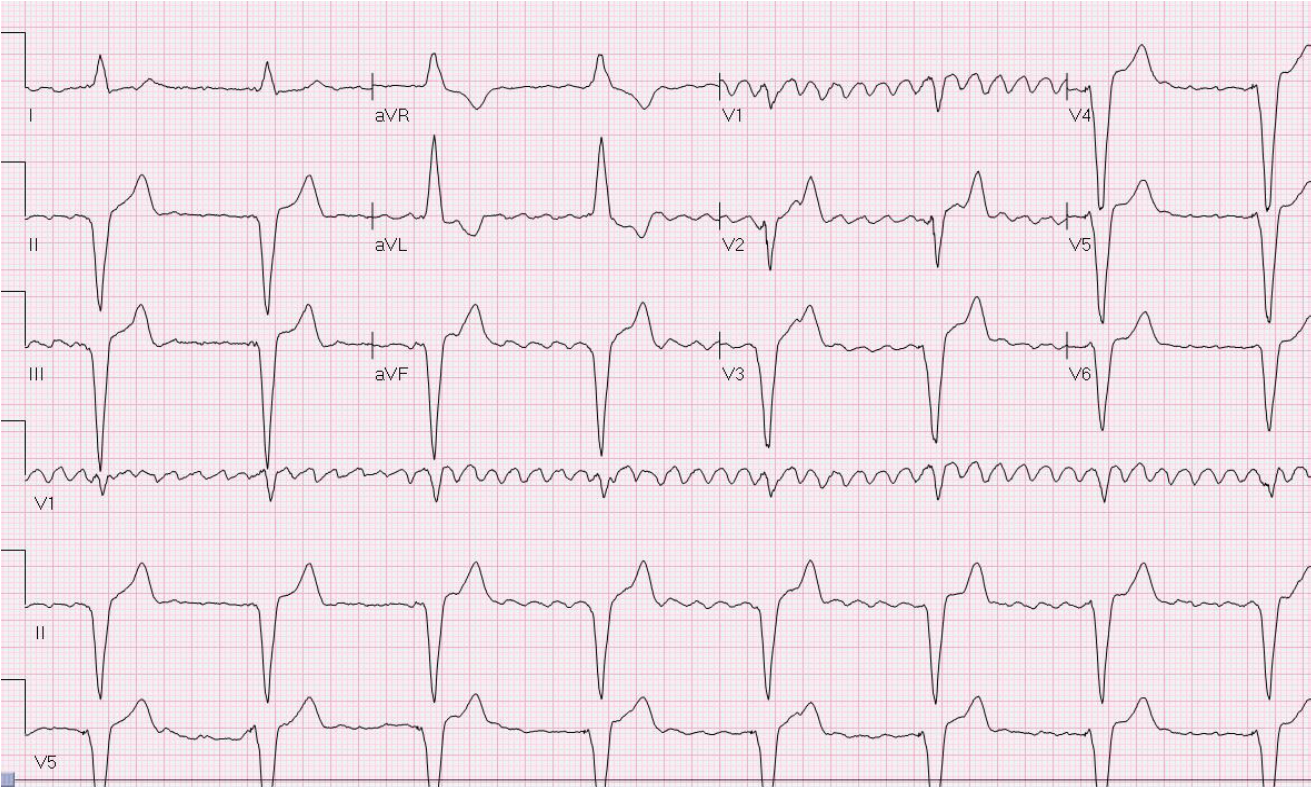
Telemetry Workshop (level 1) by Dr. D. Kagal & Dr. I. Tiong
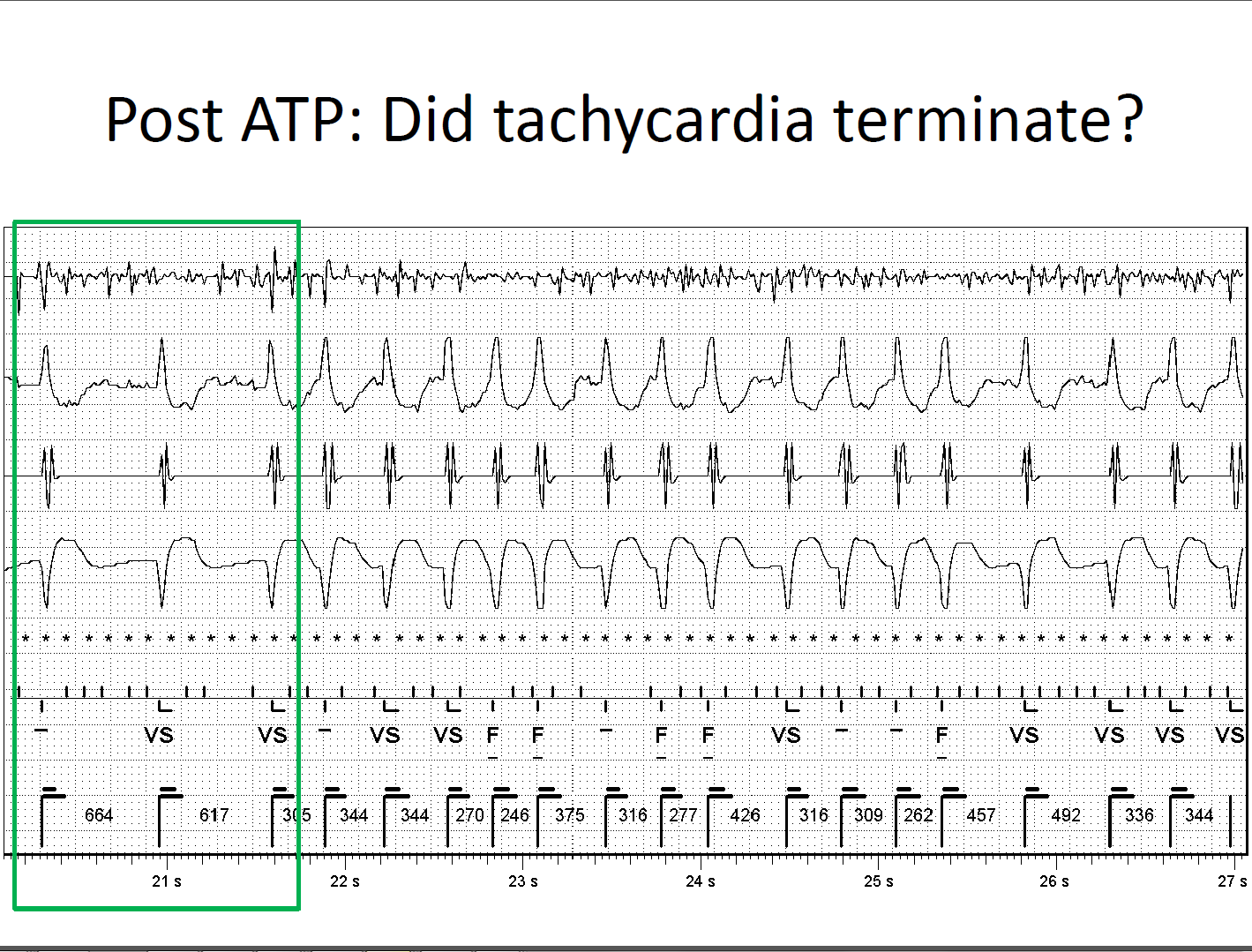
Telemetry Workshop (level 2) by Dr. D. Kagal & Dr. I. Tiong
Telemetry Workshop (level 3) by Dr. D. Kagal & Dr. I. Tiong
Intracardiac Echo – ICE, AcuNav by Dr. E. Camus
Managing Cardiac Devices at End of Life: Our Clinic’s Role in Proactive Care by
D. Campbell
Post Traumatic Stress in the Cardiac Patient by Dr. B. Baker
Post Implantable Defibrillator Shock Psychology Counselling by Dr. B. Baker
How to Become a Successful Researcher in Cardiology by Dr. M. Hartleib
Challenging Arrhythmia Cases by Dr. B. Makanjee
Pacemaker Troubleshooting (case-based) by Dr. D. Ng
Challenging Arrhythmia Cases by Dr. D. Ng
What is the Strategy of Ablation After STAR AF Trial by Dr. G. Amit
“Robotics in Ablation of Atrial Fibrillation” & “V-drive: Benefits and Challenges From User Perspective” by Dr. W. Spear
Indications for PVC Ablation by Dr. G. Nair
Duelling “PVI vs. Pace and Ablate” by Dr. G. Nair
Role of Stress Test in Arrhythmia Management by Dr. J. Healey
Magnet Application on “CIEDs” by Dr. D. Yung
Substrate Mapping Techniques and Technologies by Dr. D. Burkhardt
Robotics for Ischemic/structural VTs: Practical Tips and Tricks by Dr. D. Burkhardt
Post Implantation Wound Care by S. Turner
Duelling “Antiarrhythmic vs. Ablation of VT” by Dr. D. Burkhardt
Myths and Facts: A Discussion of MRI Imaging for Pacemaker and ICD Patients by M. Reitzel
Best Abstract Presenters
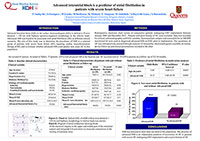
First Place went to Fariha Sadiq Ali for “Advanced Interatrial Block Predicts New Onset Atrial Fibrillation in Patients with Severe Heart Failure and Cardiac Resynchronization Therapy”.
Second Place went to Philippa Krahn for “Intrinsic Magnetic Resonance Characterization of Acute Ventricular RF Ablation Lesions”.

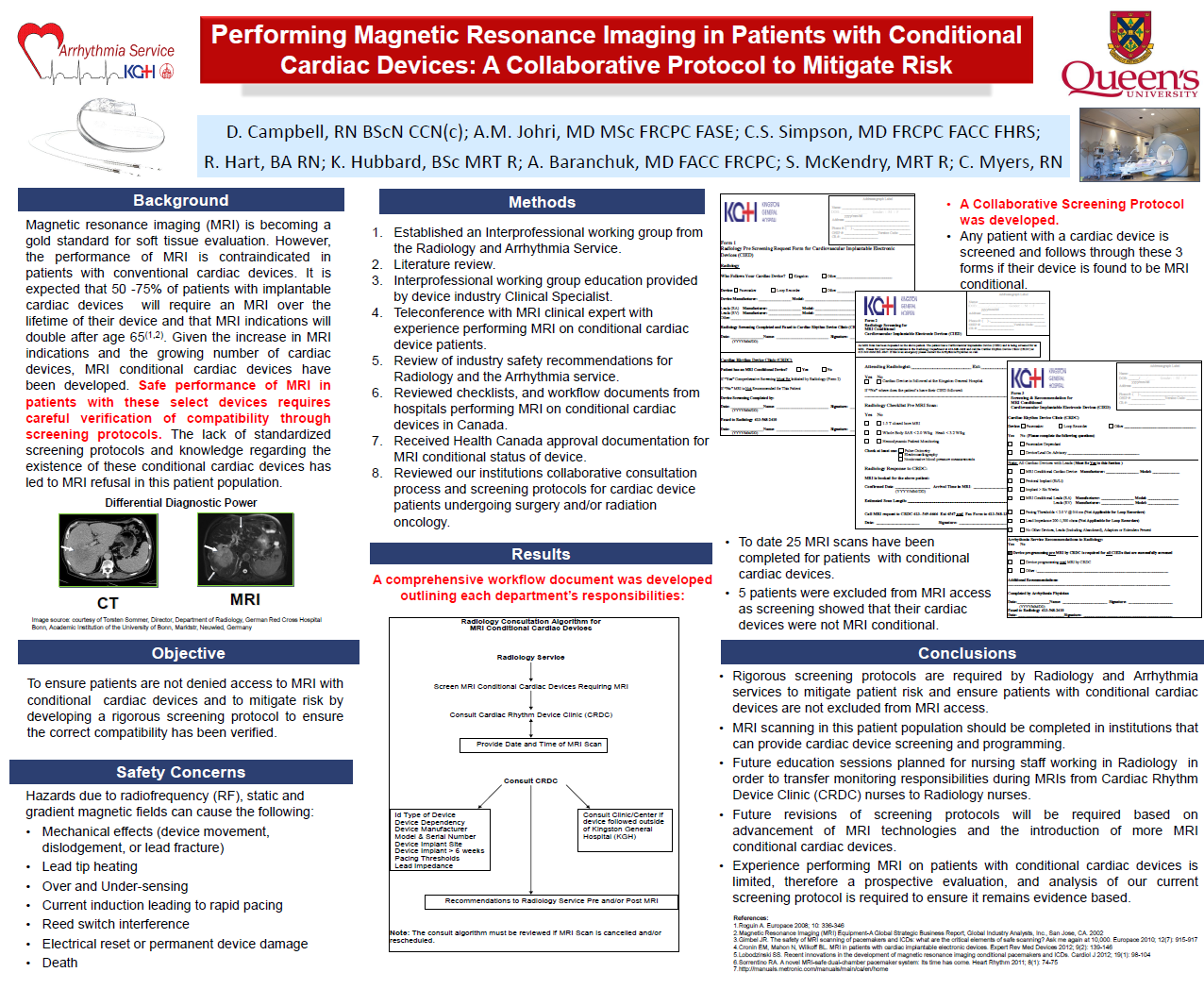
Third Place went to Debra Campbell for “Performing Magnetic Resonance Imaging in Patients with Conditional Cardiac Devices: A Collaborative Protocol to Mitigate Risk”.